

Treating Adenomyosis: From IUDs to Surgery Explained
Explore adenomyosis treatment methods including IUDs and surgeries. Learn which approach is best for pain, bleeding, and fertility.
12 minute read
Read moreDiscover how Lotus can guide you toward lasting relief.
Explore why patients choose Lotus
Search expert-written answers, browse by topic, or find information based on where you are in your journey.
Explore All KnowledgeReach out and start your healing journey.
Schedule an AppointmentClarify how adenomyosis presents and overlaps with endometriosis. Find evidence-based and integrative strategies to ease pelvic pain, guide diagnostic discussions, and personalize treatment for everyday life.
Adenomyosis most often shows up as heavy or prolonged periods, intense cramping, pelvic pressure, and pain with sex. Because the disease lives within the uterine muscle, an enlarged, tender uterus and anemia from heavy bleeding are common. Symptoms can overlap with endometriosis—pelvic pain, bowel or bladder flares, and back pain—so many people have both. Understanding the uterine‑focused nature of adenomyosis helps explain why bleeding and “deep ache” are so prominent.
Care focuses on lowering bleeding and pain, restoring energy, and aligning treatment with life goals such as fertility. Options range from NSAIDs and tranexamic acid to hormonal therapies like the levonorgestrel IUD, continuous pills, or progestins; short courses of GnRH analogs may help select cases. Pelvic floor therapy, heat, TENS, and lifestyle strategies can reduce flares and improve function. Imaging helps confirm pattern and severity to tailor care—diffuse versus focal disease may respond differently. Explore related guidance in Imaging & Diagnosis (MRI, Ultrasound), Focal Adenomyosis, Diffuse Adenomyosis, Surgical Options, Pelvic Floor PT, Anti-Inflammatory Diet, and Fertility Considerations.
Menstrual flow is generally “too heavy” when it consistently disrupts your life or overwhelms your usual period products—think flooding or soaking through pads/tampons quickly, passing frequent or large clots, needing to double up, or bleeding long enough that you can’t plan around it. Another major clue is fatigue, dizziness, or shortness of breath that can come with iron deficiency from ongoing blood loss. If you’re timing your day around bathrooms, waking at night to change products, or avoiding work, exercise, travel, or sex because of bleeding, that’s not something we consider “normal.”
Heavy bleeding is a symptom, not a diagnosis, and common underlying drivers include adenomyosis, fibroids, hormonal imbalance, and sometimes endometriosis—especially when heavy bleeding shows up with severe cramps or deep pelvic pain. Because imaging and symptoms don’t always match (a scan can look “mild” while symptoms are intense), we take a symptom-led approach and look at the full pattern, including pain, pressure, clots, cycle timing, and any signs of anemia. If your bleeding feels like it’s escalating or you’ve been told to “just live with it,” our team can help you sort out likely causes and build a plan that targets the source—not just the bleeding.
Yes—endometriosis can be associated with arthritis-like joint pain in some people, even though joint pain isn’t considered a classic “core” symptom. Endometriosis can drive chronic inflammation and immune dysregulation, and that whole-body inflammatory state may show up as aching, stiffness, or flares that feel similar to inflammatory arthritis. Some patients also notice joint symptoms that cycle with their period or worsen during broader endometriosis flares.
At the same time, endometriosis doesn’t “equal” autoimmune arthritis, and an association doesn’t prove that one causes the other. Research suggests higher rates of certain autoimmune conditions in people with endometriosis—including inflammatory diseases that can affect joints—so persistent joint pain deserves a full-picture evaluation rather than being automatically attributed to pelvic disease alone. If you’re dealing with pelvic pain plus joint symptoms, our team can help you sort out what fits endometriosis, what may be a related immune condition, and how that affects your treatment plan, including whether excision surgery and coordinated integrative support make sense for you.
Estrogen is one of the main hormones that drives endometrial growth. In the first half of the menstrual cycle, rising estrogen signals the endometrium to thicken and rebuild after a period, preparing the uterus for a possible pregnancy. It also influences the local immune and inflammatory environment in the uterus, which is part of why hormonal shifts can change bleeding patterns and pain.
When estrogen’s growth signals are strong—and progesterone’s “calming” effect is weaker than expected (often described as progesterone resistance)—the endometrium can behave in a more persistently inflamed, reactive way. This hormone–inflammation pattern is especially relevant in estrogen-dependent conditions like adenomyosis and endometriosis, where tissue similar to the endometrium can contribute to ongoing symptoms. If you’re trying to make sense of heavy bleeding, severe cramping, or cycle-linked pelvic pain, our team can help you connect the hormonal biology to what you’re feeling and review next steps for diagnosis and treatment.
Endometriosis flare-ups don’t have one “usual” length—some people feel a spike in symptoms for a few hours to a couple of days, while others have flares that stretch across an entire cycle window or blend into more constant pain. Many flares track with hormonal shifts (often before and during a period), but bowel, bladder, pelvic floor, or nerve-related pain can flare at different times and may not follow a neat calendar pattern.
When flares start lasting longer or happening more often, it can be a sign that multiple pain drivers are stacking—ongoing inflammation from lesions, adhesions/fibrosis that can “tether” organs, and sometimes central sensitization, where the nervous system becomes more reactive over time. That’s why symptom management alone can feel like a band-aid if active disease is still present. If you’re noticing prolonged, unpredictable, or escalating flares, our team can help you map your pattern, identify what’s likely driving it, and discuss a plan that addresses both symptom control and the underlying endometriosis.
“Endo belly” can last anywhere from a few hours to several days, and for some people it can linger longer or feel nearly constant during certain parts of the month. The duration often depends on what’s driving it for you—hormone-linked inflammation around ovulation or a period, bowel slowing/constipation, pelvic adhesions restricting organ movement, or a combination. Many patients notice it waxes and wanes, sometimes changing noticeably within the same day.
If your bloating is predictable and cyclical, that pattern can be a clue that endometriosis or adenomyosis-related inflammation is playing a major role—even when imaging looks “normal.” If it’s frequent, severe, or paired with bowel or bladder symptoms (pain with bowel movements, urinary urgency, rectal pressure), it can also suggest deeper pelvic disease or significant inflammation affecting nearby organs. Our team can help you sort out whether your “endo belly” is primarily hormonal, GI-driven, or related to pelvic disease that may benefit from targeted treatment, including excision when appropriate—reach out to schedule a consultation and we’ll map your symptoms to a clear plan.
Endometriosis itself doesn’t create a specific, recognizable “type” of blood clot you can identify just by looking. The clots you pass during a period are usually clotted menstrual blood mixed with pieces of shed uterine lining, so they can look dark red to deep brown, jelly-like, stringy, or like thicker “chunks”—and this can happen with or without endometriosis.
What matters more than appearance is the pattern that comes with it. If you’re seeing clots along with heavy or abnormal bleeding, severe or worsening period pain, pain with sex, bowel or bladder symptoms, or pelvic pain that isn’t limited to bleeding days, that combination can fit with endometriosis (and can also overlap with other conditions like adenomyosis or fibroids). If this is what you’re experiencing, our team can help you sort out the likely drivers and discuss what a thorough evaluation and long-term treatment plan can look like—including when minimally invasive excision surgery is worth considering.
Yes—endometriosis can be associated with heavier menstrual bleeding for some people, and heavier flow can come with larger clots. That said, large clots aren’t specific to endometriosis, because clotting is often a sign that bleeding is heavy enough that the body can’t “keep up” with breaking it down as it leaves the uterus.
When we hear about large clots, we also think about conditions that more directly drive heavy/prolonged uterine bleeding, especially adenomyosis and fibroids—which frequently overlap with endometriosis and can be missed if the focus stays only on pelvic pain. If you’re noticing new or worsening clotting (especially alongside severe period pain, pressure/bloating, or fatigue), our team can help you sort out whether endometriosis is part of the picture, whether there’s a uterine source of bleeding, or whether both are contributing. If you’d like, you can reach out to schedule a consultation so we can review your symptom pattern, prior imaging, and the next best steps for a clear diagnosis and durable relief.
Yes—many people can fly with an endometrioma, even a large one, but “safe” depends on your individual risk profile and symptoms. The main in-flight concern with a larger ovarian cyst is an acute complication like torsion (the ovary twisting) or, less commonly, rupture—events that can happen on any day, but feel especially stressful when you’re far from care. Cabin pressure changes aren’t known to make endometriomas expand, but dehydration, constipation, prolonged sitting, and limited access to pain control can make a pelvic pain flare much harder to manage mid-flight.
If you’re having escalating one-sided pelvic pain, significant nausea/vomiting, fevers, dizziness/faintness, or pain that suddenly becomes severe, we generally want you evaluated before you travel—those can be warning signs that change the plan. If you do fly, think through logistics that reduce strain: choose an aisle seat if possible, plan for gentle movement and hydration, and have a clear pain plan for the travel day so you’re not improvising at 30,000 feet. If the endometrioma is growing, very symptomatic, or affecting fertility planning, our team can help you map next steps—whether that’s careful monitoring, symptom control while you travel, or discussing targeted treatment options designed to treat the disease rather than just chasing flares.
Explore adenomyosis treatment methods including IUDs and surgeries. Learn which approach is best for pain, bleeding, and fertility.

Discover how adenomyosis might be diagnosed through imaging tests. Learn what to expect and understand your symptoms better.

Discover what adenomyosis is, why it's often overlooked, and treatment options. Understand its symptoms and relation to endometriosis.

Explore the effectiveness of supplements and herbal medicines for endometriosis and adenomyosis. What does the evidence say?
Learn what a focal adenomyosis diagnosis means, how TVUS and MRI confirm it, and your options—from medical therapy to uterus‑sparing procedures and hysterectomy.

We break down an 18‑month follow‑up of hormone therapy for adenomyosis: who was studied, symptom trends, ultrasound changes, side effects, and key limitations.
Explore types of endometriosis pain, evaluation, and evidence-based treatments, including triggers, pelvic floor therapy, CNS sensitization, and adenomyosis.
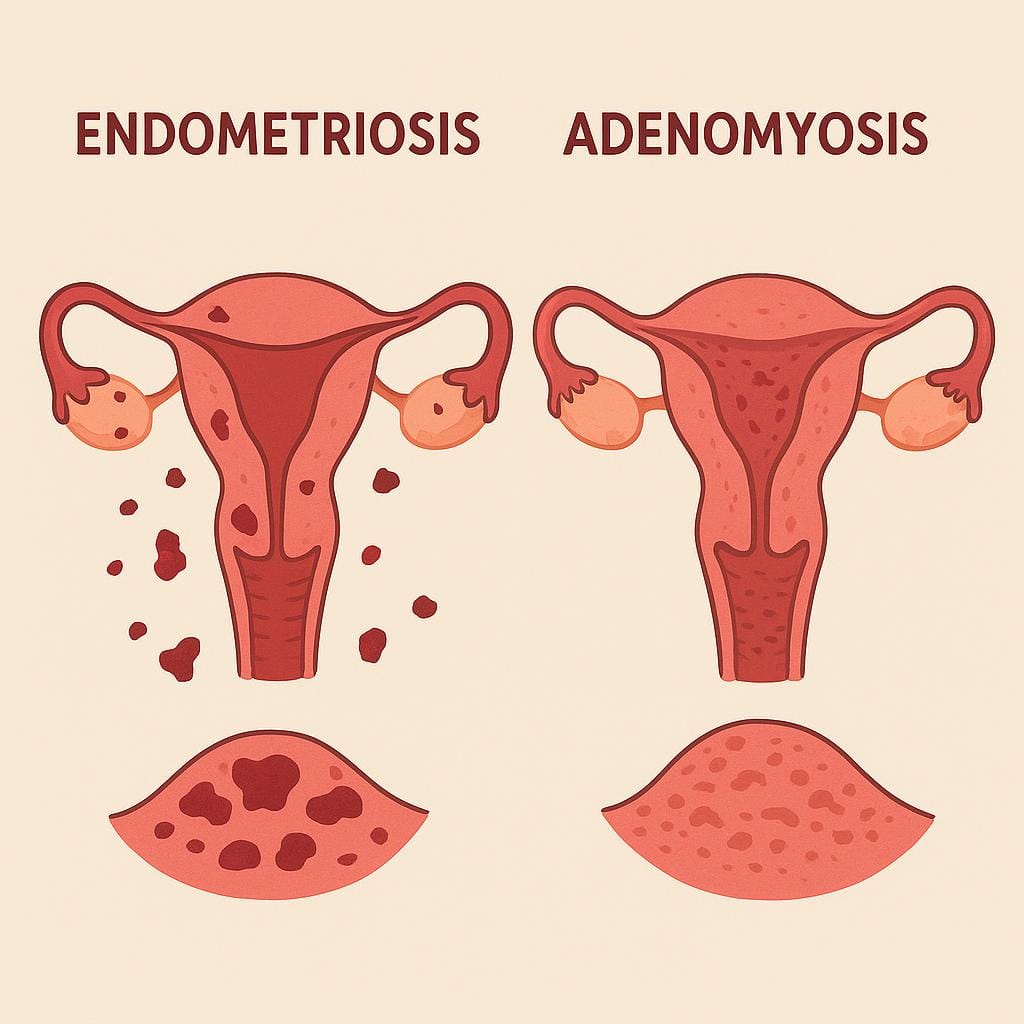
Compare endometriosis and adenomyosis: similarities, differences in location and prevalence, diagnosis methods, and treatment options for pelvic pain.
A whole-person approach to reducing endometriosis and adenomyosis symptoms, supporting healing, and improving quality of life.
Lotus Endometriosis Institute provides California-based surgical evaluation and advanced excision care for patients with suspected endometriosis, adenomyosis, complex pelvic pain, and related conditions.
Many patients contact us from outside California to learn whether traveling for in-person evaluation and possible surgery may be appropriate.
2121 Santa Monica Blvd, Santa Monica, CA 90404
8am - 5pm
Monday - Friday
154 Traffic Way, Arroyo Grande, CA 93420