


Diaphragmatic Endometriosis: Symptoms and Treatment Options
Causes, symptoms, diagnosis, treatment, and complications—explained in depth.
Diaphragmatic Endometriosis: An Overview
Diaphragmatic endometriosis is a chronic condition that occurs when tissue similar to the endometrial lining grows outside the uterus. These endometrial-like deposits commonly affect the ovaries, fallopian tubes, and bladder, but may also appear in less typical locations such as the diaphragm, upper abdominal organs like the stomach, and retroperitoneal structures including lymph nodes and kidneys. Among these uncommon sites, the diaphragm is perhaps the most frequently involved.
Understanding the Diaphragm
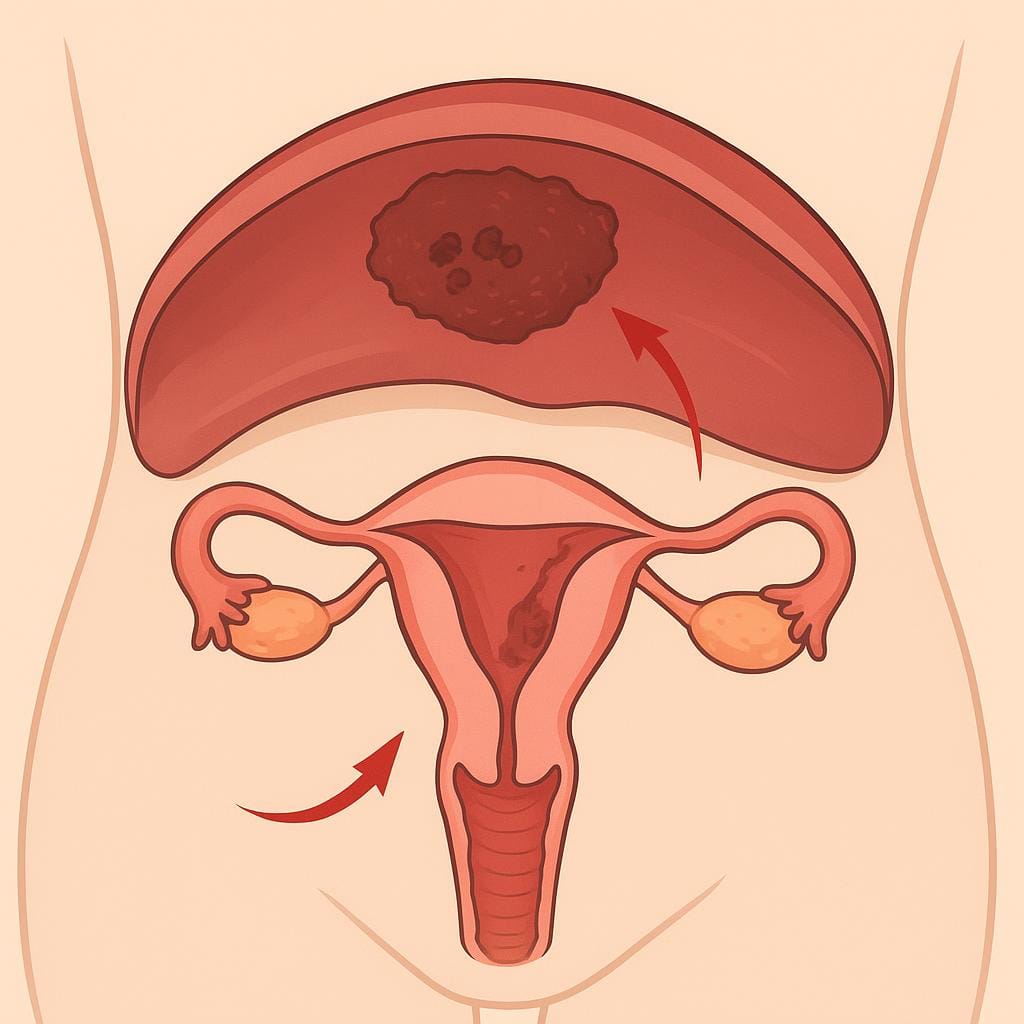
The diaphragm is a large, dome-shaped muscle located beneath the lungs that is essential for respiration. It separates the abdominal and thoracic (chest) cavities, and its involuntary contractions and relaxations facilitate breathing. The diaphragm also contains openings that allow the esophagus and major blood vessels to pass through.
What Is Diaphragmatic Endometriosis?
Diaphragmatic endometriosis most often affects the right side of the diaphragm. When endometrium-like tissue builds up on the peritoneal surface of the diaphragm, it responds to menstrual cycle hormones similarly to uterine endometrium, which can generate various symptoms.
Symptoms of Diaphragmatic Endometriosis
Typical symptoms include pain in the chest, upper abdomen, right shoulder, and arm, often around the time of menstruation. This pain may intensify with deep breathing or coughing. In rare instances, when the disease penetrates the diaphragm and involves the lungs, it can lead to a collapsed lung known as catamenial pneumothorax. Diaphragmatic endometriosis can also be asymptomatic, especially when only small superficial implants are present. For this reason, surgery generally includes at least visual inspection of the diaphragms to document the presence of any implants, even in the absence of local symptoms.
Causes of Diaphragmatic Endometriosis
The precise cause of diaphragmatic endometriosis, as with other forms of endometriosis, remains unknown. It is plausible that cells originating in the pelvis can travel through the abdomen to the diaphragm, although the factors that enable them to implant and grow there are not understood. Other possible mechanisms include spread via lymphatic channels or the bloodstream, direct transformation of stem cells, or the growth of embryologic remnants into endometriosis implants. These pathways are likely influenced by genetic and genomic molecular signaling, which is only now being more fully appreciated and unraveled.
Struggling with Diaphragmatic Pain?
Our specialists are here to help you understand your condition and explore your treatment options.
Book Your ConsultationDiagnosis of Diaphragmatic Endometriosis
Diagnosis can be challenging and often relies on a combination of medical history, physical examination, and imaging such as CT (computed tomography) or MRI (magnetic resonance imaging). The most reliable diagnostic method is minimally invasive laparoscopic or robotic surgery. Ideally, the surgeon excising pelvic endometriosis can also remove diaphragmatic implants, or a qualified surgeon should be available as part of the surgical team to do so. In the much rarer situation where endometriosis is suspected inside the chest or on or within the lungs, consultation with a thoracic surgeon is recommended.
Treatment of Diaphragmatic Endometriosis
Surgery is the primary treatment and is usually performed via minimally invasive laparoscopic or robotic techniques. The excision surgeon or surgical team should be equipped to remove endometriosis from the diaphragms. If diaphragmatic involvement is not suspected and safe excision cannot be accomplished by the available surgeons, it is best to refrain from proceeding to avoid causing more harm than good. Because the diaphragm is very thin, entering the chest can occur during excision; in expert hands, this is manageable. However, if there is uncertainty about whether the disease crosses into the chest cavity, the safest approach is to pause, obtain appropriate imaging and consultations, and plan surgery later with a thoracic surgeon.
Possible Complications
In relatively rare cases, diaphragmatic endometriosis can cause defects or holes in the diaphragm. Endometrial tissue may then extend into the chest and potentially involve the lungs, which can result in life-threatening events such as a collapsed lung during menstruation (catamenial pneumothorax) or significant bleeding into the chest that compresses the lung.
Conclusion
Although relatively uncommon, endometriosis can affect the diaphragm and, under more rare circumstances, extend into the chest and lungs. Expert endometriosis consultation and care are always advisable, and they become crucial if you experience upper abdominal or chest symptoms like those described in this article.
Quick Answers
What is pelvic dissection in endometriosis surgery?
Pelvic dissection in endometriosis surgery means carefully separating and opening tissue planes in the pelvis so we can clearly see normal anatomy and remove disease safely. Endometriosis can cause inflammation and scarring that “glues” organs together (sometimes called a frozen pelvis), so dissection is often the step where we free adhesions and restore normal relationships between the uterus, ovaries, bowel, bladder, and pelvic sidewalls.
In practical terms, pelvic dissection may include identifying and protecting critical structures like the ureters, bladder, bowel, blood vessels, and pelvic nerves before excising endometriosis at its roots. This is where surgical precision matters: the goal is to fully address disease while minimizing injury to healthy tissue, especially in complex or re-operative cases. If you’re seeing this term on an op note or surgical plan, it usually reflects the complexity of the anatomy and the deliberate work needed to make excision both complete and safe—our team can walk you through exactly what was dissected and why in your specific case.
What does a frozen pelvis mean with endometriosis?
A “frozen pelvis” isn’t a separate diagnosis—it’s a descriptive term surgeons use when the uterus is essentially stuck in place because endometriosis-related inflammation has caused dense scarring (adhesions). Instead of the uterus moving freely, it may be tethered to nearby structures like the bowel, bladder, ovaries, or pelvic sidewall, sometimes pulling the uterus into an abnormal position and making pelvic anatomy hard to distinguish. Thus some have also called it a "frozen uterus".
This finding often suggests more advanced disease, such as deep infiltrating endometriosis and/or significant adhesions from prior inflammation or surgery, and it can help explain symptoms like deep pelvic pain, painful sex, bowel or bladder symptoms, or pain that doesn’t match what a routine exam shows. In these cases, surgery is less about “burning spots” and more about carefully restoring normal anatomy—freeing organs, protecting ureters and bowel, and removing endometriosis at its roots. If you’ve been told your uterus is “frozen,” our team can help you understand what that implies for imaging, surgical planning, and which adjacent organs may need to be evaluated as part of a complete excision strategy.
Can endometriosis spread to the brain?
Yes—endometriosis can occur outside the pelvis, and it has been reported in distant parts of the body. That said, brain involvement is extremely rare compared with pelvic disease or even other extra‑pelvic locations like the diaphragm and chest.
When people worry about “endo in the brain,” it’s often because they’re experiencing neurologic symptoms (headaches, nerve-type pain, numbness/weakness) that seem to flare with their cycle. Sometimes those symptoms are related to endometriosis affecting nerves or areas higher in the abdomen/chest rather than the brain itself, and the cyclical timing can be an important clue. If you have unusual symptoms that track with menstruation, our team can help you think through the full-body picture, determine what’s most likely, and map out next steps for accurate diagnosis and treatment—including minimally invasive excision when appropriate.
Can a ruptured ovarian cyst cause severe pelvic pain?
Yes. A ruptured ovarian cyst can cause sudden, severe pelvic pain—often sharp and one-sided—and it may be intense enough to feel alarming, especially if there’s internal bleeding or irritation of the lining of the pelvis. Some people also notice nausea, shoulder-tip pain, dizziness, or pain that worsens with movement, while others have a milder ache that fades over hours to days.
Because pelvic pain has many look-alikes and coexisting causes (including endometriosis, adenomyosis, ovarian/paraovarian cysts, torsion, bladder pain, or pelvic floor spasm), what matters is the pattern of your symptoms, your exam, and correctly interpreted imaging like ultrasound or MRI when appropriate. Our team focuses on sorting out whether a cyst rupture is the whole story—or one piece of a bigger picture—so you’re not stuck treating the wrong problem. If you’re having severe pain, recurrent “cyst” episodes, or pain that tracks with your cycle, reach out to schedule an evaluation so we can pinpoint the driver and map out next steps.
What are signs endometriosis has returned after surgery?
Endometriosis “returning” after surgery can show up as symptoms that improve for a while and then gradually (or suddenly) come back months or even years later. The most common signal is the return of your familiar pattern—cyclical pelvic pain, worsening period pain, pain with intercourse, or pain that starts spreading beyond where it used to be. Some people also notice bowel or bladder symptoms re-emerge (pain with bowel movements, rectal pressure, urinary urgency or bladder pain), especially if those organs were involved before. New or increasing fatigue and activity limitation can be part of the picture, but the key is a clear change from your post-op baseline.
It’s also important to know that recurrent pain doesn’t always equal recurrent disease. Even after complete excision, the nervous system can stay “turned up,” and pelvic floor dysfunction, adhesions, or central sensitization can keep pain going or make normal sensations feel painful—so we think in terms of patterns, triggers, and timing rather than a single pain score. If symptoms are returning, our team can help you sort whether you’re in a true recurrence lane (improved, then returned) versus persistent pain that never fully settled, and decide when imaging (such as ultrasound or MRI) is useful—particularly for tracking ovarian endometriomas. If you’re noticing a shift back toward your old symptoms, reach out to schedule a consultation so we can build a clear, long-term follow-up plan with you.